Lead in paragraph that is long enough to make the drop cap work. I don’t care what anyone says, I like drop caps.
the difficult is, you see, days and months can go by when nothing changes. I could post endless variations of “I woke up, ate breakfast, then sat around the house doing nothing until it was time for bed again” but I don’t think that’s what my audience wants.
So I am forcing myself to write about something. This week has not been great. The symptom du jour is anhedonia which has meant I haven’t really wanted to talk to anyone about anything, ever. So of course this was the week I had three people reach out wanting to chat. Which I would love to do, if my brain could figure out how to break out of this funk.
I was going to write in a bit more detail about how the funk is hitting me this time but instead, I’m going to bed.
I started out intending this to be about all the outlandish assumptions my brain tries to function under. Instead, its going to be about how difficult it is for me to accept help, or even praise.
First, it has come to my attention there were a few people unaware of the existence of this blog until now. For anyone in that class, I apologize. It was not a deliberate oversight, when I started this thing I thought I had mentioned it to anyone who might be interested. I was apparently wrong. Not in that the people who I missed weren’t going to be interested, I just missed some people somehow. Anyway, welcome to whatever this is.
Back to the actual topic of this post.
It is very difficult for me to accept help, or praise.
Thank you for your attention.
Edited to add: It has been longer since I looked at this blog than it has been for many of the people reading this so, out of morbid curiosity, I went back to start reading some of the older posts. I can’t do it. I started reading them and was okay until I started hitting posts about covid. Looking those over was not a good idea. Lesson learned
Edited further to add: The thing is, I’m kind of interested to go through those posts because I really don’t remember much detail at all between about March of 2020 and sometime in 2023.
Among the happenings over the last year was being denied social security disability benefits. In spite of opinions to the contrary provided by my actual care providers, SSDI felt there was no reason I couldn’t “adapt to other work”. The nature of the “other work” was not specified.
I had tried, over the preceding 16 months or so, to not count on getting disability benefits. I knew it was a long shot, at least the first time around, but I also didn’t have a long-term Plan B. This has not contributed anything to my peace of mind.
The Plan B I was pretending I had, and which I don’t think was really fooling anyone, involved me sucking it up and going back to work. What with my preexisting doubt there is anything really wrong with me in the first place (well documented in previous posts) and social security insisting I could adjust to other work, I tried hard to resign myself to the idea of returning to hospital nursing. Several incidents of greater or lesser significance over the last few months have persuaded me this isn’t realistic, in spite of any protestations I might make to the contrary.
As one might infer from the numbers in the previous post, I remain symptomatic. I still don’t know what to do with myself when panic-brain takes over, which happens much too frequently in spite of everything. Dr. Psychiatrist is still experimenting, trying to find some combination of meds to make me a bit more functional. which is a process I am trying to not get discouraged about as well.
Am I better than I was this time last year? Probably? But certainly not better enough.
If anyone is likely to have some sort of RSS or whatever the latest subscription/reader/feed application is on this site, its you. So hi.
My MHP (mental health professional, for those not in the know) suggested I should share more information with the people around me. I have been assured this will be therapeutic for me and appreciated by the people around me. I remain unconvinced on either point, fortunately the chances of anyone actually reading this are negligible so off we go.
Very little has changed since the last post, made over a year ago. Read that one and make of the situation what you will.
Oh look! This place is still here! I am not going to bother trying to summarize what went on over the last year beyond saying, things have continued to be a little closer to the “Dumpster Fire” end of the scale than I’m happy with.
I am, as we speak (read? type? communicate?), unemployed. I left my non-patient care job at Swedish and started an actual clinical education job at the University of Washington hospital. Unfortunately, the environment was still much too hospital-y for my anxiety and I was having almost daily panic attacks at work again. I’m not at all sure what this bodes for my future employment, but I’m still looking. I’m branching out to non-hospital jobs but the one offer I’ve had so far paid less than I was making 10 years ago. So no. I could write a great deal about the experience of applying, and being denied unemployment benefits, but that may be for another day.
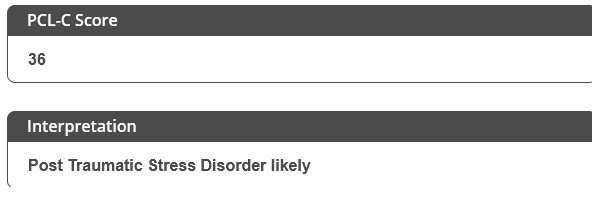
The other big development over the last year has been an increasing difficulty being out and about in the world. It seems that people with PTSD and other panic disorders are prone to develop symptoms of agoraphobia. Who knew?
My symptoms aren’t so bad that I can’t leave the house, but they do kick in when I’m around crowds, especially if I have to stand in a line and wait. The checkout line at a busy grocery store is just about guaranteed to make me go sideways.
I’m not sure what this means for the future. I’m not sure if this is a permanent thing. I do know that it’s kind of a pain in the ass.
A couple of things I don’t think I’ve mentioned here have cropped up again today. Among the reasons I took the job I currently have was the medical benefits kicked in on my hire date. None of this “the first of the month after your first full month of employment” nonsense, sign to accept the job; get benefits. At least that’s what I was told and, to be fair, that was probably the intention of my employer. Unfortunately it didn’t exactly work out that way.
I’ll spare the reader the blow-by-blow details of what happened but the short version is, for reasons that no one can adequately explain, Shannon did not get added to my medical and dental coverage. It took three weeks of fighting with the benefits people and me turning in my resignation for it to get fixed. I did withdraw my resignation after being promised the insurance would be fixed (by sheer coincidence this promise came almost immediately after me submitting my resignation). Anyway, as of yesterday it was supposed to be all fixed.
Imagine my surprise, then, when we got a message from our pharmacy saying there was a problem with the insurance, which is exactly what they said when we found out about the problem in the first place. Fortunately it turned out to be a relatively common and easily corrected SNAFU with the pharmacy’s records but the situation still put me very much on edge again, which is what I really came to talk about.
I have previously talked a fair amount of shit about trigger warnings. It isn’t that I object to their use, nor do I have any doubt that trauma-related disorders can result in certain otherwise normal everyday events and topics to be distressing for people. What I object to is the use they have commonly been put to in discussion forums and the like, which is to put responsibility for one person’s mental health on to someone else – “OMG I am so triggered right now!How dare you not put trigger warnings on your completely ordinary and generally uncontroversial content? Now my triggers have been triggered and its your fault for triggering me because you didn’t use trigger warnings which has resulted in me being very triggered by the triggers you failed to warn me about“.
So this is the difficulty I’m running into. It is hard to talk about the things that escalate my stress and anxiety, “triggers” if you will, without sounding like a complete choad. This gets right back to my baseline difficulty with mental health in general; the overwhelming majority of my professional experience with mental health has been with people ostentatiously using a, usually self-diagnosed, mental health condition as an excuse to behave like a raging asshole. This is a particularly sensitive topic for me right now because my own mental health condition has resulted in me behaving kind of like a raging asshole over the past few weeks.
I don’t know what the solution to this is. My worst fear… among my worst fears is becoming one of those people who may as well have their diagnosis tattooed on their forehead and who use it as a central piece of their personality and all their social interactions. Meeting someone for the first time? Better make sure you work the fact that you’re neurodivergent into the conversation in the first few sentences, no matter how tangential it may be to the topic at hand, to make sure everyone knows you’re different and interesting. On the other hand, if simple things are going to elevate my stress and anxiety it might be a good idea to let people know.
In 2000 the Institute of Medicine published To Err is Human: Building a Safer Health System, a landmark work that shone the light, really for the first time, on the incidence and severity of medical errors. Why do I mention this? Because I’m pretty sure I had one.
As seen in the previous post, for the last few weeks I’ve still been having panic attacks and was quite symptomatic with depression and anxiety which prompted Dr. Primary Care to start me on sertraline. While I was seeing Dr. Primary Care I also got a refill on my bupropion since I was nearly out. I started the newly refilled prescription yesterday and noticed something kind of odd.
I want to take a moment here to mention I am aware of the difficulties and pitfalls of identifying pills by sight. Pills from different manufacturers will look different even if they are the same drug and the same dose. That said, I’ve seen quite a few pills in my day and I can generally spot things that are different because of manufacturer and things that are genuinely off.
So I started my newly refilled prescription and noticed that the new pills were markedly larger than the ones I had previously been taking, in spite of appearing to be from the same manufacturer. By chance I have access to examples of 150 mg XL tablets in addition to the 300 mg XL tablets that I am supposed to be taking and I am as certain as I can be without any physical evidence that the pharmacy filled my last prescription for 300 mg XL with 150 mg XL.
Two additional pieces of evidence that could add weight to the theory; once I started taking my new 300 mg XL tablets I immediately started feeling better. My mind has not been this calm in weeks and my overall mood has improved a great deal. Also when I started taking my new 300 mg XL tablets, I was struck with a serious case of insomnia which is a common side effect of bupropion. It hasn’t really been a problem for me1 except for a couple of days after a dose increase.
There are potentially confounding factors to consider however. As mentioned above, I don’t have any physical evidence. All I have is an empty bottle that says 300 mg XL, and a comparison of my mental image of the pills I was taking to known samples of 150mg and 300mg tablets that appear to be, but can’t be said for certain to have, come from the same manufacturer. There is also the addition of sertraline to my regimen. I’ve been on it for a week and, while usually SSRIs take a bit longer to really take full effect, the possibility that I’m just feeling the benefit of the sertraline cannot be ruled out. Finally, the insomnia could very easily have resulted from me working my first full week on night shift after being on a “sleep when you want, wake up when you want” schedule for a couple months.
Pretty sure but not certain.
The thought of the difficulties I’ve been having with my mood over the past few weeks being the result of a medication error is actually reassuring to me. I was feeling distraught because I thought I’d been making all this progress in therapy and introspection and self-analysis and all, but here I was feeling like shit most of the time again. Additionally, if this was a medication error, any doubt about the benefit of being on medication that I may have had is gone. Being on a half-dose was all kinds of no fun so I don’t even want to think what being off it entirely would be like at this point.
1 I know, I know. But there is my baseline insomnia and then extra insomnia gets piled on top of it. Insomniaception. A couple of days after my last increase in dosage I was back to my baseline insomnia.
As previously mentioned, I had a cast on my dominant hand for the last few weeks. This condition didn’t make typing or writing impossible but it did make both activities more frustrating than was tolerable for anything less than absolute necessity. Astute readers will doubtless have reached the conclusion that, since this post was typed out by me, and nothing I do here is even in the same neighborhood as anything even remotely necessary, I must be out of the cast now. This is, in fact, the case. Dr. Ortho-Hand was satisfied enough with how the fracture had healed that he didn’t even feel the need to put my in a removable splint. I have an entirely bare naked hand and, in spite of my wrist feeling like it tried to fuse solid and is now only grudgingly moving again, I could not be happier with the situation.
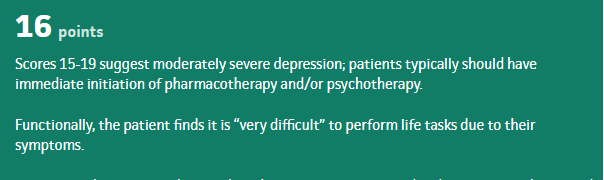
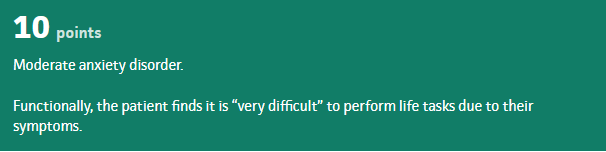
On the topic of not being happier2, astute readers may also have reached the conclusion that, based on the title of this post, my prescribing provider and I have been messing around with the medications again. My PHQ-9 and GAD-7 scores3 have been getting uncomfortably high again and I have still been having panic attacks multiple times per week4. Fortunately my health insurance situation has stabilized and I was able to go back to the primary care provider I had been seeing for several years prior to starting my whirlwind tour of employers. Given the degree to which I have been symptomatic, Dr. Primary Care felt that adding a serotonergic antidepressant would be beneficial. I have been on sertraline twice previously and we’re at 50/50 in terms of it being effective. I did, however, tolerate it well as far as side effects go so that’s where Dr. Primary Care felt we should start5.
One of the complaints I have with antidepressants is they can take a ridiculously long time to really take effect, weeks in some cases, so it may be difficult to tell if any improvement is from the medication or from me just settling back into a work/school routine with a lower baseline stress level.
On the topic of work6, I have started my new, non-patient care job and I feel like it will be okay once my nervous system adjust to the idea of me going to work in a hospital but NOT going to work in an ICU filled with people dying from a pandemic respiratory virus. I’ll talk more about work later (probably) but for now I’m going to go eat some tylenol and rest my wrist.
1 Apologies to Lennon/McCartney
2 How’s that for a transition!
3 Patient Health Questionnaire and Generalized Anxiety Disorder scales for assessing depression and anxiety symptoms. These are a desperate attempt to put an objective measure on the extremely subjective experience of emotional distress. They’ve been validated in peer-reviewed studies and people more knowledgeable on the topic than myself rely on them, so ¯\_(ツ)_/¯
4 I don’t want to leave people with the impression that I’m getting worse. I still think I’m improving in general but “better” is not the same as “well” unfortunately.
5 For those keeping score at home, this brings the total number of prescription psych meds I’m taking to three.
I spent most of the time between Tuesday morning and Thursday night last week having what felt like one, very long panic attack. Of course I didn’t recognize it as a panic attack until it was over. I seem to have two flavors of panic attack but neither of them have the precise textbook presentation I learned in school; a feeling of impending doom or a fear of death, frequently physical symptom similar to a heart attack, etc. What I seem to get are a sense that everything in the world in general and my life in particular is broken and nothing will ever be able to fix it, or a sense that everyone in my life either hates me or is angry with me about something. The one under discussion was the former and I spammed several friends, family members, and my therapist with texts and emails about how it wasn’t fair how badly my life sucked and now we’re going to have World War III thanks to Putin.
The thing is, at the time I did not feel irrational and, in my defense, it really has been a few pretty rough years and the nature of my reaction wasn’t completely unjustified. The problem started when my (perfectly justified) dissatisfaction with the state of the world turned into an out of control semi barreling downhill with no breaks. On some level I knew something was wrong. I knew I didn’t feel like myself, I couldn’t think clearly. It felt like my brain just wasn’t working right.
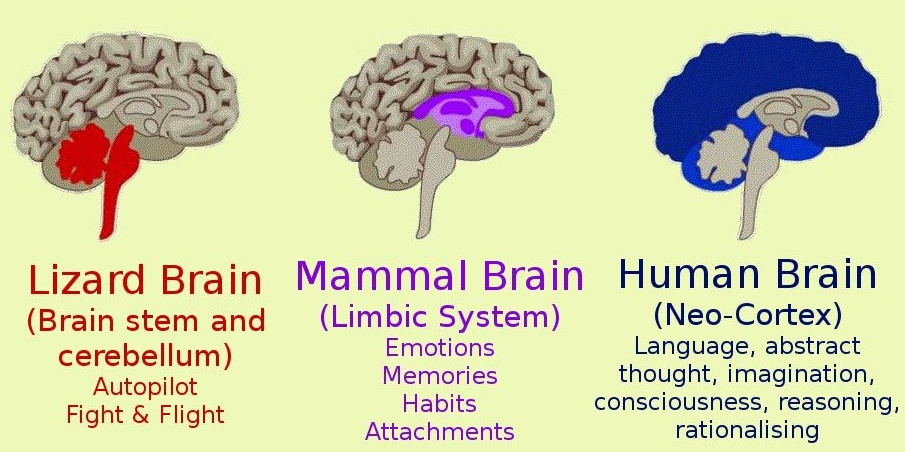
At this point I would like to pause for a moment and talk about brain anatomy. In broad terms, the human brain can be divided into three sections, the brainstem, the limbic system, and the cortex.
what a brain might look like
Generally, the brainstem tells you that you’re hungry and need food, the limbic systems tells you to go find food, and the cortex decides whether you want Thai or Mexican. Or, more importantly, tells you that you can’t go look for food right now because other things are more important.
That inhibitory function of the cortex is the key. The brainstem starts shouting about how there’s a big problem here (whatever it might be, probably a saber-tooth tiger), the limbic system agrees that this is a big problem (whatever it is and we certainly can’t rule out the tiger theory) and we’d better do something about it right fucking now. It is at this point where the cortex is supposed to step in and remind everyone that saber-tooth tigers have been extinct for a really long time now and all that happened was some jerk cut us off in traffic.
Problems start because under enough stress, either intensity or duration, the limbic system kind of stops talking to the cortex. It decides that the big problem (whatever it is) is important enough that we have to deal with it and we don’t have time for the guys at headquarters to get back to us. This effectively removes the filter between thought and action which frequently results in people doing stupid things like spamming their friends with apocalyptic text messages.
Or punching a wall.
What I’m learning is it’s impossible to think yourself out of a panic attack because the thinking part of your brain is quite literally not at the controls anymore. Of course the goal would be to not have panic attacks in the first place which is why I’m also trying very hard to learn the warning signs so I can do something to change the situation before the lunatics take over the asylum as it were. Unfortunately I am really bad at recognizing the warning signs, partly because I’ve spent the overwhelming majority of my life not just ignoring them but desperately pretending they didn’t exist at all. Since nothing my limbic system could do would get the attention of my cortex to have it fix the problem, my limbic system decided it needed to turn things up to a point where they couldn’t be ignored anymore.
The point to all this is I will almost certainly have more panic attacks in the future and people may very well see me behaving somewhat erratically. Be assured that in a matter of hours, or a couple days at most, I’ll be fine so just strap in and hang on.