Once again exposing some bias or another1 in my thinking, I assumed everyone knew what the PHQ-9, GAD-7, and PCL-C were and how they worked. I may have even explained here at some point. or maybe I didn’t…
Anyway, the point is, I want to give a quick explanation of what they are and how they work.
All three of these are screening tools for various mental health diagnoses. The Patient Health Questionnaire-9 (nine questions) and Generalized Anxiety Disorder-7 (seven questions) especially were designed for primary care providers to use to screen all their patients for depression and anxiety. The PCL-C2 is the civilian version of the PTSD screening tool developed by the military to screen troops. They rely on the frequency of symptoms like anhedonia, feelings of isolation or disconnection from others, nightmares, etc. as reported by patients. They were designed to be used by health care professionals and their patients in the setting of a therapeutic assessment. They were never intended to be self-administered, and certainly not self-interpreted. I am, in short, using them wrong3 and the numbers may or may not mean anything.
They’ve been scientifically validated and are relied upon by experts in the field so I’m more or less obligated to accept them as valid. When used as intended. I tend to have fairly concrete thinking when it comes to health care so having any kind of number to look at makes things easier. Whether or not the numbers are actually useful is a different question.
I’ve never been clear on which of my many neuroses causes this to happen but for whatever reason I commonly assume that if I know something, everyone else must know it too. It was something I was consciously trying to change when I was working on my education degree and have, clearly, fallen out of the habit. ↩︎
I’ll be honest, I have no idea what this stands for and I’m not going to bother to look it up. ↩︎
Considering the disdain I hold for people who use the internet to diagnose themselves with various things, this may come off a bit hypocritical. I thread that needle in my mind by asserting my (still valid) credentials as a health care professional and that these are being used in the setting of receiving treatment for the relevant disorders. Hopefully I can swing a bit more nuance than someone lacking the appropriate organs diagnosing themselves with uterine fibroids. ↩︎
I spent most of the time between Tuesday morning and Thursday night last week having what felt like one, very long panic attack. Of course I didn’t recognize it as a panic attack until it was over. I seem to have two flavors of panic attack but neither of them have the precise textbook presentation I learned in school; a feeling of impending doom or a fear of death, frequently physical symptom similar to a heart attack, etc. What I seem to get are a sense that everything in the world in general and my life in particular is broken and nothing will ever be able to fix it, or a sense that everyone in my life either hates me or is angry with me about something. The one under discussion was the former and I spammed several friends, family members, and my therapist with texts and emails about how it wasn’t fair how badly my life sucked and now we’re going to have World War III thanks to Putin.
The thing is, at the time I did not feel irrational and, in my defense, it really has been a few pretty rough years and the nature of my reaction wasn’t completely unjustified. The problem started when my (perfectly justified) dissatisfaction with the state of the world turned into an out of control semi barreling downhill with no breaks. On some level I knew something was wrong. I knew I didn’t feel like myself, I couldn’t think clearly. It felt like my brain just wasn’t working right.
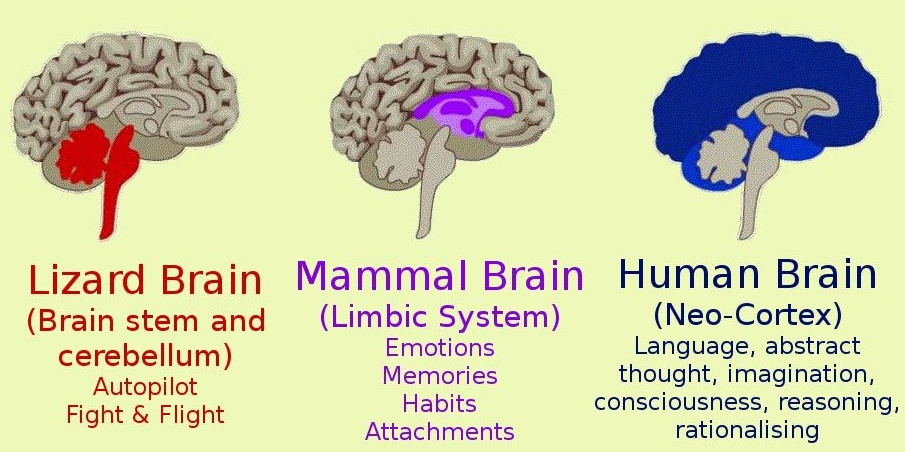
At this point I would like to pause for a moment and talk about brain anatomy. In broad terms, the human brain can be divided into three sections, the brainstem, the limbic system, and the cortex.
what a brain might look like
Generally, the brainstem tells you that you’re hungry and need food, the limbic systems tells you to go find food, and the cortex decides whether you want Thai or Mexican. Or, more importantly, tells you that you can’t go look for food right now because other things are more important.
That inhibitory function of the cortex is the key. The brainstem starts shouting about how there’s a big problem here (whatever it might be, probably a saber-tooth tiger), the limbic system agrees that this is a big problem (whatever it is and we certainly can’t rule out the tiger theory) and we’d better do something about it right fucking now. It is at this point where the cortex is supposed to step in and remind everyone that saber-tooth tigers have been extinct for a really long time now and all that happened was some jerk cut us off in traffic.
Problems start because under enough stress, either intensity or duration, the limbic system kind of stops talking to the cortex. It decides that the big problem (whatever it is) is important enough that we have to deal with it and we don’t have time for the guys at headquarters to get back to us. This effectively removes the filter between thought and action which frequently results in people doing stupid things like spamming their friends with apocalyptic text messages.
Or punching a wall.
What I’m learning is it’s impossible to think yourself out of a panic attack because the thinking part of your brain is quite literally not at the controls anymore. Of course the goal would be to not have panic attacks in the first place which is why I’m also trying very hard to learn the warning signs so I can do something to change the situation before the lunatics take over the asylum as it were. Unfortunately I am really bad at recognizing the warning signs, partly because I’ve spent the overwhelming majority of my life not just ignoring them but desperately pretending they didn’t exist at all. Since nothing my limbic system could do would get the attention of my cortex to have it fix the problem, my limbic system decided it needed to turn things up to a point where they couldn’t be ignored anymore.
The point to all this is I will almost certainly have more panic attacks in the future and people may very well see me behaving somewhat erratically. Be assured that in a matter of hours, or a couple days at most, I’ll be fine so just strap in and hang on.
More commonly known as clonidine. Clonidine is an alpha-adrenergic agonist, and should not be confused with clonazepam (Klonopin) which is a benzodiazepine. As was previously mentioned, I had an appointment with Dr. Rando and among the things she recommended was adding a medication for anxiety to the antidepressant I’m already taking. Discussed options included benzodiazepines (which are not recommended for use in PTSD1), beta-blockers (which she was hesitant to put me on since I had been having issues with fatigue), prazosin (which is also an alpha blocker but is only indicated to treat nightmares associated with PTSD2), and clonidine.
TL; DR – I started on clonidine and I feel like it’s working really well. My baseline level of nervous system jangling has dropped noticeably. You are now safe to skip the rest of this post which consists of some rambling about how clonidine works, why I was positively enthusiastic to try it, and how irrational the distinction I have in my head between “psychiatric” medications and “physical” medications is.
My reaction to the suggestion of more medication highlights again my physical medicine bias. I resisted being on an antidepressant for a long time, and even after I started one initially my goal was to get off it as soon as possible (and then resisted going back on one when it looked like it was going to be required). However, when Dr. Rando suggested clonidine I was positively enthusiastic for a couple of different reasons. First, I am well familiar with clonidine. It was a mainstay medication for our ECMO program because it (at least theoretically) has beneficial effects on pain control, sedation, and blood pressure, it is available as a pill that can easily be crushed, dissolved, and put down a feeding tube if the patient can’t swallow, and, perhaps most importantly to the Powers-That-Be, it is dirt cheap. I understand how it works and, because I know how it works, I could see how it would help with the difficulties I have been having. The other reason I was enthusiastic to try it was the opportunity to see first hand if it really did work the way it was supposed to.
I want to talk a bit about exactly how irrational it is that I would resist adding, say, an SSRI to treat PTSD while not only accepting but being enthusiastic about trying clonidine. As I mentioned above, clonidine is an alpha-adrenergic agonist, which means that it inhibits some of the fight-flight-or-freeze response that our nervous system does when it feels threatened. In past times this response was a great adaptation because it allowed our progenitors to run away from saber-toothed tigers. In modern times it can be maladaptive because modern life is very good at creating stress that one can’t fight or run away from so the stimulation of our nervous system doesn’t turn off. Ever. The practical effect of using an alpha-blocker to moderate the activation of our nervous system is to reduce the hyper-alert state, resulting in improvement in tension and anxiety. Clonidine can do this by having the ability to cross the blood-brain barrier3 and by being structurally similar to norepinephrine, one of the main neurotransmitters in our nervous system. In terms of it’s mechanism of action, it is essentially indistinguishable from most medications that have primarily psychiatric indications.
Of course none of that matters to my brain. It’s a medication that I have used and am familiar with, and it has primarily physical indications which means it’s a real medication and not one of those woo-woo brain drugs (that work in extremely similar ways to achieve similar effects). Totally irrational.
This is one occasion on which I will not complain about my brain behaving irrationally. Whatever the reason I was able to persuade my brain that this was a necessity, I’m very pleased with how the medication is working so far. It has settled my nervous system sufficiently to make every day life a great deal less challenging.
There is more to catch up on but I am taking advantage of the reduction in mental clutter to enjoy doing things. What kind of things? Almost anything really. Even doing chores around the house is less troublesome when you aren’t spending an excessive amount of energy trying to keep from having a complete breakdown.
1 I’m not entirely sure why benzodiazepines aren’t indicated for PTSD. I suspect it has something to do with benzos having the potential to be disassociative which, based on my extremely limited understanding, is probably counterproductive.
2 I have no idea why one alpha blocker (prazosin) is only indicated to treat nightmares and another alpha blocker (clonidine) is indicated for general symptom treatment. Seriously, no clue.
3 I also don’t know enough about the blood-brain barrier to even attempt to explain it, so here’s Wikipedia.
Those among the none people visiting this site who do so exclusively for all the cancer talk may be in for a bit of disappointment in the next weeks to months. Cancer is still a thing, I will still be getting treatments, and I will still be writing about them here but what is top of mind right now, as odd as it seems, is not cancer. If me droning on about mental and emotional health is not of interest, you may want to check back later.
I have a blind spot when it comes to mental health1. This has come up before but I want to highlight one manifestation of this blind spot in particular. I touched on the thought process that my brain went through regarding my ability (or inability) to work briefly in a previous post and the same pattern applies more generally as well. In order to explain the behaviors I see in myself while avoiding the conclusion that those behaviors are the result of mental health factors I may not have complete control over requires some quite startling twists of logic, and accepting, without question, the assumptions necessary to make those twists is, I think, a large part of the problem.
What the fuck am I talking about? Let me offer an example;
I’ve been irritable recently1. Things of little to no consequence have been getting under my skin to an exceedingly disproportionate degree. I like to think I’m a rational person who doesn’t let emotion influence my decision making. Let’s run through the thought process I used to make all of those things be true and a little bit of the consequences of the necessary assumptions:
I am a rational person
I am getting irritated over trivial things, which isn’t rational
I must be consciously choosing to get irritated because I don’t let emotion influence what I do
Wait, isn’t choosing to be irritated even more irrational? There must be a reason I’m doing this
I must be trying to manipulate people in to thinking I’m getting irritated so they’ll think the pressure and stress are getting to me and I’ll have an excuse to not work
Why do I need an excuse to not work? I like my job, I enjoy being a nurse, and since I’m immune to the physical and mental consequences of stress, it must just be that I’m lazy and don’t want to work
Wow. So I’m feigning mental illness just to get out of work? I must be a really terrible person. I really need to stop doing that
I’ve tried but I can’t seem to stop pretending I’m disproportionately irritable, therefore I am both lazier and more of a terrible person than I even realized.
For comparison, the process I’ve been working with more recently is as follows:
I haven’t been able to stop being a terrible person and drop the pretense that I have some sort of incipient mental health issue because I actually have an incipient mental health issue and all the things I’ve been “pretending” to do are actual symptoms
Also, it isn’t so much “incipient” as it is “fully armed and operational”
Upon reflection, what this reminds me of most is a well known headline from The Onion:
Or in my case, why can’t I stop pretending to have PTSD?
Anyway, excluding any other analysis, Occam’s Razor would lead one to suspect that the latter chain of reasoning was correct over the former, and it also has the benefit of not requiring me to be a totally shit human being in order to be true.
Which is, of course, why my brain keeps telling me it can’t possibly be true. It seems I’m just trying to let myself off the hook and rationalize my ongoing terrible behavior. After all, if I believe it’s a genuine mental health issue I won’t have to give it up, stop being a lazy-ass, and go back to work. My brain, as has been mentioned, is not terribly helpful sometimes.
If one accepts the unlikely premise that spending the last two years working in an ICU during the worst pandemic in a century may have had an impact on my mental health, comfort can be taken in the knowledge that I am far from alone. Caillet et al. (2020)2 found the incidence of anxiety and depression among ICU caregivers were 48% and 16%, respectively, and PTSD symptoms were present in 27% of respondents. That was as of September and I suspect those numbers have not improved3.
I can’t say how this is all going to play out in the larger context but brought down to the level of one individual (if that individual happens to be me) I can make what I think are some very accurate short-term predictions.
But that is a story for another day.
1 This is the equivalent of saying the Pacific Ocean gets quite deep in some bits.
2 Caillet, A., Coste, C., Sanchez, R., & Allaouchiche, B. (2020). Psychological Impact of COVID-19 on ICU Caregivers. Anaesthesia, critical care & pain medicine, 39(6), 717–722. https://doi.org/10.1016/j.accpm.2020.08.006
This in-line citation is really problematic. What kind of maniac has both in-line citations and endnotes? This is exactly the kind of societal collapse I’ve been warning about. My only excuse is that my school uses APA format (in-line citations) and virtually all the journals and whatnot I read use AMA (endnotes). That said, no excuse can justify this. I’m a monster.
3 The only reason I’m even a little uncertain about the current rates of depression, anxiety, and PTSD being worse or better is I can’t exclude the possibility that all the people predisposed to those conditions have already washed out which would make the percentages look better in spite of the overall situation being worse.
I stumbled across this kind of randomly while wandering around the internets and, for a couple different reasons, thought I should share it.
As mentioned previously, I’ve had the pandemic right up in my face pretty much since the beginning. I’ve watched it spread, wax, wane, wax again and, most significantly I think, I’ve dealt with essentially nothing else in my professional life. My therapist pointed out to me recently that when you’re that close to something, it tends to look very large. Sometimes disproportionately so.
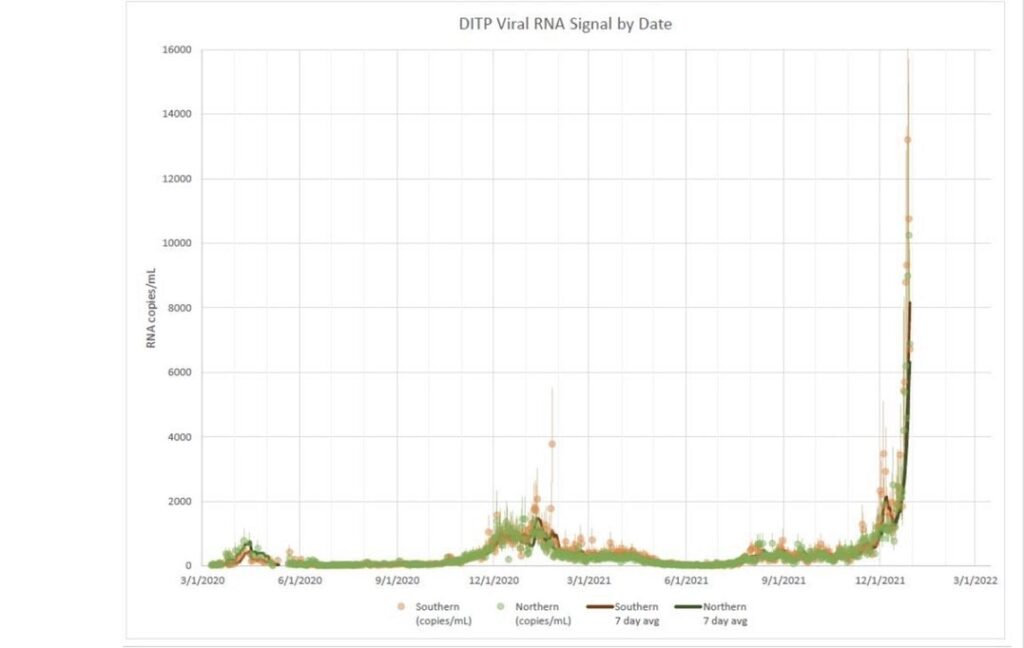
I am by no means downplaying what’s going on. We’re still really not in a good place when in comes to case numbers, rate of spread, and available hospital resources. Models are predicting that the omicron surge will peak in 2-3 weeks with close to 1,000,000 new cases per day in the United States. Keep in mind, too, that the official counts are still, very likely, drastically undercounting. This graph is wastewater analysis from Boston showing the increase in viral DNA in sewage. The spike from omicron completely obliterates the spikes from all the other surges we’ve seen so far suggesting that there are likely significantly more cases than have been recognized;
All that said, we have come a long way from the beginning and there is still hope that we can survive this with something that looks more or less like modern society relatively intact.
Now we come to what brought me here today;
“Your Local Epidemiologist (YLE)” is written by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, biostatistician, professor, researcher, wife, and mom of two little girls. During the day she has a research lab and teaches graduate-level courses, but at night she writes this newsletter. Her main goal is to “translate” the ever-evolving public health science so that people will be well equipped to make evidence-based decisions, rather than decisions based in fear.
The most recent newsletter is entitled “There is good news” and is worth a read. Things are bad but they could be worse and they will get better. Eventually.
Anyway, read it and feel some momentary relief from the doom that I’ve been spouting.
One of the more common objections to the covid vaccine is that no one who claims to be a Good Christian™ (and it’s always Christians) can get the vaccine because it was made using “aborted fetuses”.
As anyone with more than two functioning neurons could guess, reality is a bit more complicated. The Oxford-AstraZenica vaccine was, in fact, developed using Human Embryonic Kidney 293 (HEK-293) cells. These cells are commonly used to replicate viral proteins which are then used to deliver mRNA sequences. The HEK-293 cells themselves are not a part of the finished products.
“But wait,” you might say, “If the AstraZenica vaccine is the only one that is manufactured using HEK-293 cells, why don’t they just take one of the other ones?” Well here’s the thing, HEK-293 cells are also frequently used in the early stages of development to test the function and potential toxicity of a new drug, and every single one of the covid vaccines was tested on HEK-293 cells. What can a Good Christian™ do but decline to take these vaccines that were tested on the cloned cells of an immortalized cell line originally derived from the kidneys of a fetus that was either aborted or miscarried, no one is quite sure which, in 1973 poor innocent murdered babies.
The problem is that there are a METRIC CRAPTON (2.2 imperial craptons) of drugs that are tested for safety using HEK-293 cells.
(Blatantly stolen from https://www.patheos.com/blogs/throughcatholiclenses/2021/01/if-any-drug-tested-on-hek-293-is-immoral-goodbye-modern-medicine/)
Common over the counter medicines tested on HEK-293 cells or derivative cell lines.
Take particular note, if you will, of numbers 12 and 15 on the list of prescription medications and you may spot some familiar names if you’ve been following the trends in quack covid treatments.
Essentially, if Good Christians™ are going to take a moral stand against being vaccinated because of their opposition to abortion, they’re pretty much going to have to give up on modern medicine. Fortunately, at least one employer is asking anyone requesting a religious exemption from the vaccine to do just that.
If it’s a sincerely held belief, you have to be consistent, right?