There is a possibility that I’m overgeneralizing somewhat with this, and I may also be doing some post-hoc revisions of my internal dialogue. That said, what follows feels true to me and has allowed me to resolve some very perplexing things that my brain has been doing.
For some time now I have been having a harder time than usual with work. I’ve been finding it increasingly difficult to go to work in the first place and once I’m there I have a really hard time staying. This is not an entirely new phenomenon, and is also not unique to me. Who looks forward to going to work and who is happy to be there once they arrive? Almost no one, that’s who. That said, this has felt very different than the usual vague malaise of dissatisfaction that comes from having to put down Animal Crossing and leave the house.
“Well of course you’re having problems,” you might say, “you’ve been in cancer treatment and dealing with fatigue from that. No one expects you to be at the top of your form!”
This is true. I have a very real physical medical condition and I have unquestionably been experiencing some physical side effects from my treatment. However, at this point there really isn’t any reason that these side effects should be as limiting as they appear to be and, if I’m completely honest, they probably aren’t as limiting as I have been allowing them to be.
As I have discussed here previously, my brain constantly tells me that I am malingering or exploiting the system somehow because, in terms of physical health, I likely could be working without any restrictions right now. The slow realization that there might not be an actual physical problem sapping my willpower and energy has kicked the “you’re just a lazy bastard” message from my brain into overdrive in the last few weeks
Again, though, I genuinely have been feeling like I’m incapable of working, and the worst scolding from my brain hasn’t made it any easier to keep pushing and just do the work, so WTF?
At this juncture it is important for the narrative that I mention my longstanding prejudice when it comes to mental health. My poor opinion results from long years of dealing with the healthcare consuming public, which certainly has no shortage of people with genuine, serious issues, but also no shortage of people just trying to game the system. The way my mind works, it comes down to Sick or Not-Sick. You can’t objectively measure depression, anxiety, and trauma so they probably aren’t real. Intellectually I know this is nonsense and when it comes to patients I try hard to stay aware of this bias and to not let it affect the care I provide.
When it comes to myself, though, it is something of a blind spot. Deep down, I don’t completely accept the notion that my mental health is a real thing that can actually affect how I approach the world. Again, intellectually I know this is nonsense but that seems to be how my brain wants to see things.
Keeping all that in mind, my thought process has been something like the following;
Stage 1
- The only valid reasons for me being unable to work are physical ones.
- I’ve been feeling very limited in my ability to work.
- Therefore, something must be physically wrong with me.
Stage 2
- The only valid reasons for me being unable to work are physical ones.
- I don’t physically feel all that bad, really.
- I still appear to be limited in my ability to work.
- Therefore, I must be faking it.
Stage 3
- The only valid reasons for me being unable to work are physical ones.
- I still don’t physically feel all that bad, really
- I still appear to be limited in my ability to work.
- This doesn’t feel at all like I’m faking it.
- ???
The explanation, of course, is that my first assumption is faulty. I really am limited in my ability to work but at this point it’s for mostly psychological and emotional reasons, not physical.
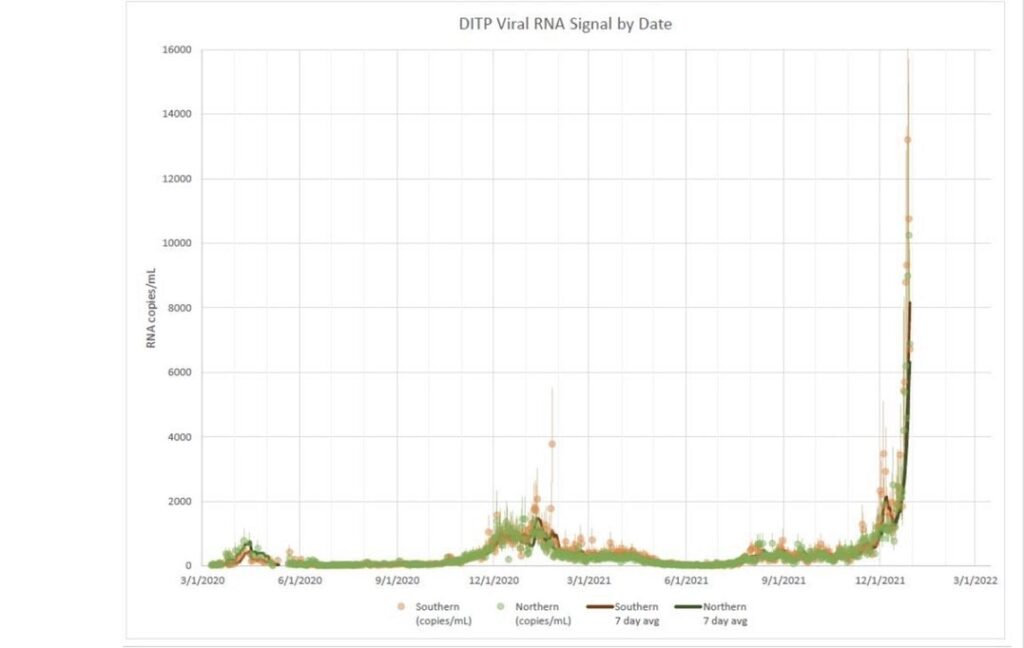
In February of 2020, an emergency room doctor at Evergreen Medical Center in Kirkland was infected with Covid. His condition deteriorated quickly and he was transferred out of the ICU at Evergreen to Swedish Cherry Hill so he could be put on ECMO. He was the first Covid patient on the west coast, probably in the whole United States, to be put on ECMO. That was my unit and I was one of the lead ECMO specialists.
I lost count of how many more Covid patients we put on before I left Cherry Hill. They all were insanely sick1, insanely complex to care for and most of them died, as did most of the Covid patients we had that weren’t on ECMO.
This went on non-stop.
For months.
And it still hasn’t exactly stopped yet.
There was a lot of non-Covid unrest at Swedish at the time as well, of course, so I had plenty of reason to be discontent before I left. Given that mental health isn’t real, I attributed my angst to the external situation and didn’t think about it past that.
Since then I have changed jobs two more times for a total of three job changes in the last 18 months or so. Each of the jobs ended up feeling unsatisfactory for one reason or another and, like I had at Swedish, I felt compelled to leave. True, the working conditions weren’t (and aren’t) ideal but I’m also starting to think that there is an underlying current of mental disfunction that is making it nearly impossible to get comfortable and settle in.
The point is that it has been a difficult couple of years and perhaps there could be some lingering trauma that I’ll probably need to deal with at some point.
For all my airs of professionally detached objectivity, I may be merely human after all.
Looking after my mental health has never been one of my strong suits but entertaining the idea that I could be mentally fatigued enough to impact my job performance has been something of an eye-opener. It explains a great deal of what I’ve been experiencing and it has already helped me to get the asshole part of my brain to shut up every now and then. Beyond that, I’m not sure if this shift in thinking will make any difference or not.
This post was very long and has an unsatisfying conclusion. It also may not matter because, hopefully, I will be changing jobs again in the near future.
But that is a story for another day.
————
1 I’ve talked about this before too, although I can’t remember if it was here. I don’t think it’s possible to convey the actual reality of how sick these patients were/are to normal (non-medical) people. Even most medical people, I think, fail to grasp how sick they are. The best analogy I’ve come up with is that caring for these patients is like trying to keep someone who is on fire alive but you have to do it without being able to extinguish them. I love doing that kind of work but it is exhausting under the best of circumstances.