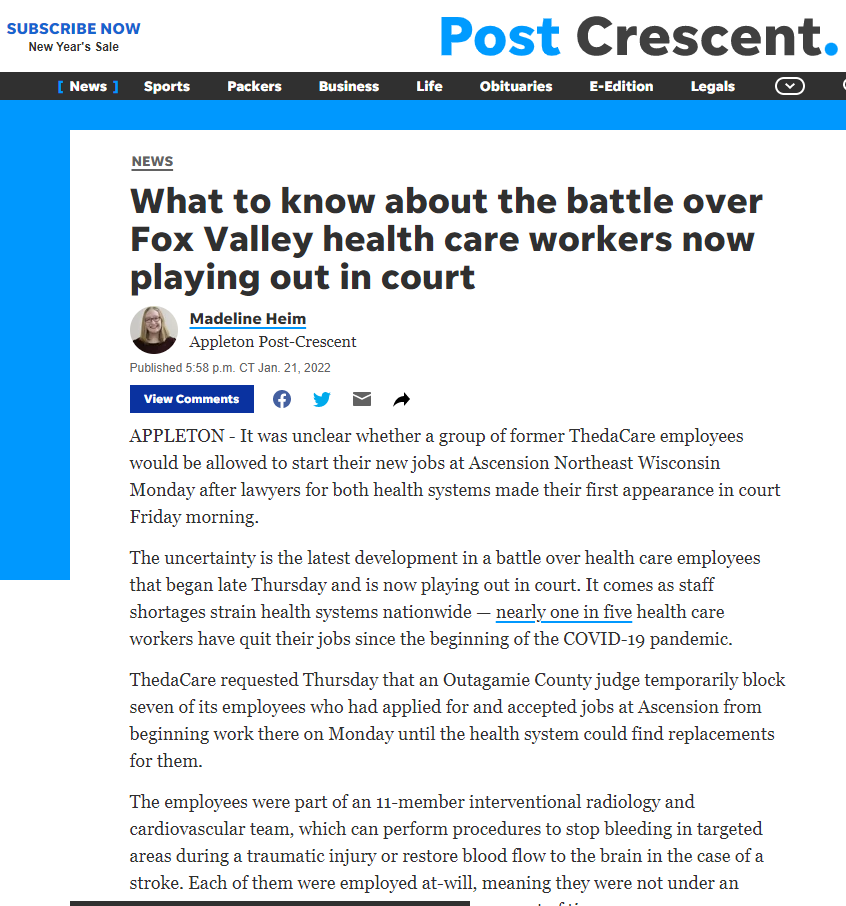
ThedaCare requested Thursday that an Outagamie County [Wisconsin] judge temporarily block seven of its employees who had applied for and accepted jobs at Ascension from beginning work there on Monday until the health system could find replacements for them.
The employees were part of an 11-member interventional radiology and cardiovascular team, which can perform procedures to stop bleeding in targeted areas during a traumatic injury or restore blood flow to the brain in the case of a stroke. Each of them were employed at-will, meaning they were not under an obligation to stay at ThedaCare for a certain amount of time.
Outagamie County Circuit Court Judge Mark McGinnis granted ThedaCare’s request and held an initial hearing Friday morning. The case will get a longer hearing at 10 a.m. Monday.
McGinnis told lawyers for both health systems they should try to work out a temporary agreement by the end of the day Friday about the employees’ status until Monday’s hearing.
Otherwise, he said, the order prohibiting them from going to work at Ascension would be final until a further ruling was made. That means the seven health care workers would not be working at either hospital on Monday.
I intended to write about this when the saga first began because I was concerned, but then I though “Ha! There’s no way a judge in an AT-WILL EMPLOYMENT STATE would tell a bunch of employees they can’t quit their job”, but here we are.
A group of highly specialized hospital employees announced en masse that they were going to leave their current AT-WILL EMPLOYER to go to another facility that paid more. “After approaching ThedaCare with the chance to match the offers they’d been given, [one of the employees] wrote that they were told ‘the long term expense to ThedaCare was not worth the short term cost,’ and no counter-offer would be made”. Instead, the hospital went to court to get an order to prevent the staff from quitting.
And it looks like they’re going to get it.
This is only a preliminary injunction and it doesn’t tell the employees they can’t quit, but it does tell them that they can’t start a new job until the legal matter is settled. There is another hearing on Monday.
Keep in mind that 51% of Americans have 3 months or less worth of savings and 25% have no savings at all. The judge can’t order the employees not to quit but he can (apparently) prevent them from taking another job. I have no doubt the current employer knows, once their employees are prevented from taking another job, all they have to do is drag out the proceedings for a few weeks to a few months and their employees will be faced with the choice of economic ruin or going back to work for them.
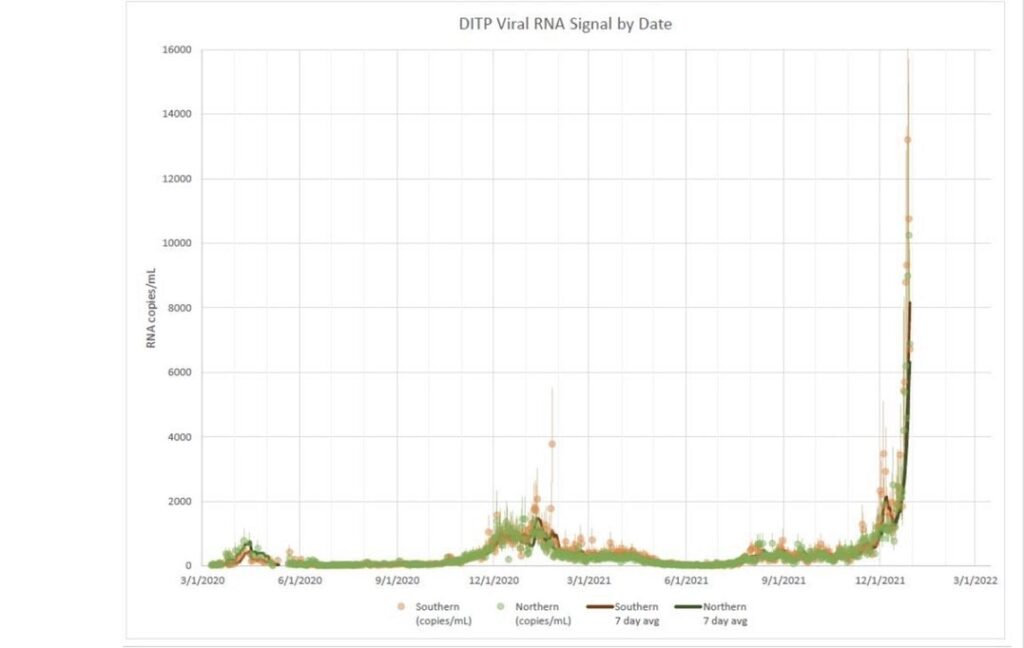
It is no secret that hospital staffing is in a major crisis right now and a lot of what is driving that is people taking the opportunity to pursue better paying jobs. The femtosecond this ruling came down, I can guarantee that hospital CEOs all over the country were waking their corporate lawyers up and telling them to get to work filing for injunctions. Why pay competitive wages when you can just get a judge to force your employees to keep working for you? Why pay them at all in fact?
I am a highly specialized, essential worker who is not currently interested in doing the job that I am highly specialized to do.
I imagine people can see why I’m concerned.